Hyperkalemia is one of the most commonly encountered electrolyte abnormalities prompting consideration of delaying/cancelling a case. There is no clear, widely accepted value at which hyperkalemia becomes "unsafe" and thus warrants cancellation. Therefore, developing a systematic approach to assess/manage this condition is critical and allows for more nuanced decision making than simply setting a threshold value without consideration for the case at hand.
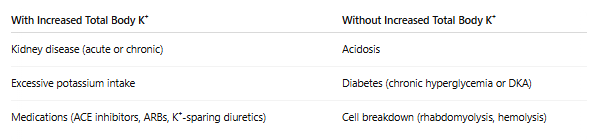
The most commonly accepted definition of hyperkalemia is serum concentrations >=5.0mEq/L, with critical values generally being >=6.5mEq/L. It is important to recognize that we are measuring serum potassium, which is a distinct entity from total body potassium. Serum potassium is only the extracellular potassium found in the bloodstream, while total body potassium also includes all of the potassium in the body, including intracellular, interstitial, etc. This distinction can become important when considering the etiology and management.
Potassium is a critical component of the maintenance of membrane resting potential, and derangements can cause widespread disruption of normal cellular function. This can cause a variety of issues, with the most pertinent to Anesthesiologists being the risk of cardiac dysfunction.
More specifically, hyperkalemia can cause cardiac dysrhythmias, ranging from benign to life-threatening. The most concerning, terminal manifestation of hyperkalemia is ventricular fibrillation, which can prove fatal if not rapidly managed.